What Is Hallux Abducto Valgus?
Overview
 Bunion is a prominence of the medial portion of the head of the 1st metatarsal bone. The cause is often variations in position of the 1st metatarsal bone or great toe, such as lateral angulation of the great toe (hallux valgus). Secondary osteoarthritis and spur formation are common. Symptoms may include pain and redness, bursitis medial to the joint, and mild synovitis. Diagnosis is usually clinical. Treatment is usually a shoe with a wide toe box, protective pads, and orthotics. For bursitis or synovitis, corticosteroid injection may be helpful.
Bunion is a prominence of the medial portion of the head of the 1st metatarsal bone. The cause is often variations in position of the 1st metatarsal bone or great toe, such as lateral angulation of the great toe (hallux valgus). Secondary osteoarthritis and spur formation are common. Symptoms may include pain and redness, bursitis medial to the joint, and mild synovitis. Diagnosis is usually clinical. Treatment is usually a shoe with a wide toe box, protective pads, and orthotics. For bursitis or synovitis, corticosteroid injection may be helpful.
Causes
Many problems that occur in the feet are the result of abnormal pressure or rubbing. One way of understanding what happens in the foot due to abnormal pressure is to view the foot simply. Our simple model of a foot is made up of hard bone covered by soft tissue that we then put a shoe on top of. Most of the symptoms that develop over time are because the skin and soft tissue are caught between the hard bone on the inside and the hard shoe on the outside. Any prominence, or bump, in the bone will make the situation even worse over the bump. Skin responds to constant rubbing and pressure by forming a callus. The soft tissues underneath the skin respond to the constant pressure and rubbing by growing thicker. Both the thick callus and the thick soft tissues under the callus are irritated and painful. The answer to decreasing the pain is to remove the pressure. The pressure can be reduced from the outside by changing the pressure from the shoes. The pressure can be reduced from the inside by surgically removing any bony prominence.
Symptoms
Symptoms, which occur at the site of the bunion, may include pain or soreness, inflammation and redness, a burning sensation, possible numbness. Symptoms occur most often when wearing shoes that crowd the toes, such as shoes with a tight toe box or high heels. This may explain why women are more likely to have symptoms than men. In addition, spending long periods of time on your feet can aggravate the symptoms of bunions.
Diagnosis
A thorough medical history and physical exam by a physician is necessary for the proper diagnosis of bunions and other foot conditions. X-rays can help confirm the diagnosis by showing the bone displacement, joint swelling, and, in some cases, the overgrowth of bone that characterizes bunions. Doctors also will consider the possibility that the joint pain is caused by or complicated by Arthritis, which causes destruction of the cartilage of the joint. Gout, which causes the accumulation of uric acid crystals in the joint. Tiny fractures of a bone in the foot or stress fractures. Infection. Your doctor may order additional tests to rule out these possibilities.
Non Surgical Treatment
Treatment options vary with the type and severity of each bunion, although identifying the deformity early in its development is important in avoiding surgery. The primary goal of most early treatment options is to relieve pressure on the bunion and halt the progression of the joint deformity. A podiatrist may recommend these treatments. Padding and Taping, Often the first step in a treatment plan, padding the bunion minimizes pain and allows the patient to continue a normal, active life. Taping helps keep the foot in a normal position, thus reducing stress and pain. Medication, Anti-inflammatory drugs and cortisone injections are often prescribed to ease the acute pain and inflammation caused by joint deformities. Physical Therapy, Often used to provide relief of the inflammation and bunion pain. Ultrasound therapy is a popular technique for treating bunions and their associated soft tissue involvement. Orthotics, Shoe inserts may be useful in controlling foot function and may reduce symptoms and prevent worsening of the deformity. 
Surgical Treatment
If non-surgical treatments have failed to relieve your bunion pain, or when the pain is interfering with your daily activities, contact the Dallas bunion surgery specialists at North Texas Foot & Ankle to discuss surgical options. There are a several ways to perform bunion surgery. The best procedure for one person is not necessarily the best for another. Some procedures allow you to walk much sooner, reducing the need for crutches. Depending on your foot type, the procedure can have a greater risk for return of the bunion deformity. Other procedures may require you to be on crutches for a few weeks - but could offer a better result in the long-term. Learn more about the different types of bunion surgery.
Over-Pronation
Overview
Pronation is a normal motion which occurs after heel strike during walking. As the foot moves towards toe off, the foot naturally should move from an outside path towards the midline of the body stopping at neutral in ideal conditions. Overpronation is the foot?s motion past neutral and moving excessively toward the bodies midline. Overpronation can be caused by a number of factors including internal rotation of the femur or thigh bone, internal torsion of the tibia or shin bone, being genu valgum or ?knock kneed?, as well as fixed deformities of the ankle and forefoot. The overpronating foot is often hypermobile meaning it has excessive range of motion in the foot joints.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
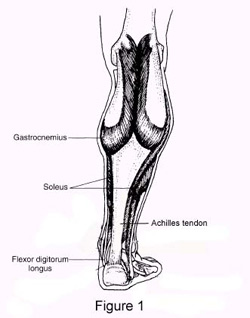
You can test for pronation by looking at the leg and foot from the back. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.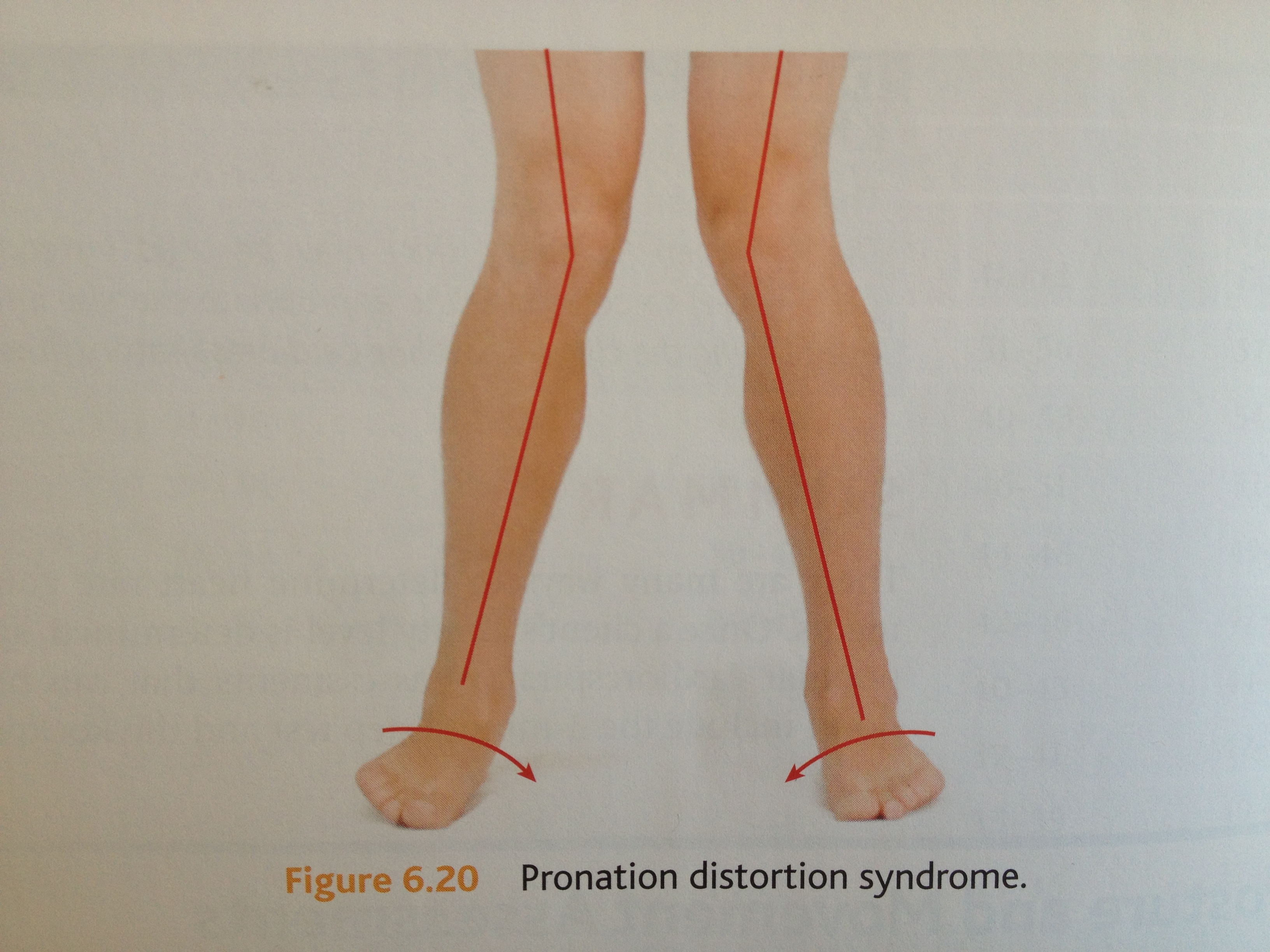
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Pronation is a normal motion which occurs after heel strike during walking. As the foot moves towards toe off, the foot naturally should move from an outside path towards the midline of the body stopping at neutral in ideal conditions. Overpronation is the foot?s motion past neutral and moving excessively toward the bodies midline. Overpronation can be caused by a number of factors including internal rotation of the femur or thigh bone, internal torsion of the tibia or shin bone, being genu valgum or ?knock kneed?, as well as fixed deformities of the ankle and forefoot. The overpronating foot is often hypermobile meaning it has excessive range of motion in the foot joints.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
You can test for pronation by looking at the leg and foot from the back. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
What Is Severs Disease?
Overview
Sever's disease, is a musculoskeletal condition occurring in adolescence that symptomatically manifests as posterior heel pain during ambulation. Often participation in physical activity is severely limited resulting in frustration for children and parents alike. Conservative treatment options have included rest, abstinence from athletic activity, heel lifts, foot orthotic devices, ice, and calf-stretching exercise. The authors are proposing arch taping as an additional viable treatment option for controlling heel pain during athletic and other weight-bearing activities in patients with Sever's disease.
Causes
Your child may have pain along the edges of one or both heels during exercise. The pain usually goes away with rest, but may be worse in the morning. Your child's heel may also be slightly swollen and warm. The heel pain may be worse when your child climbs steps or stands on tiptoe. It may cause your child to limp.
Symptoms
Pain in the bottom surface and at the back of the heel. Extreme pain when the child places their heel on the ground. The pain is aggravated when running or jumping on hard surfaces. The pain is reduced when the child walks or runs on their toes.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
In general, the goals for treatment include reducing the localized areas of inflammation. We recommend that patients utilize Ibuprofen every six to eight hours as needed. Stretching exercises on a daily basis, as well as prior to activity is thought to be helpful as well. Following work-outs and increased activities, it may be helpful to apply ice over affected areas. Heel cups are also available to provide cushion in shoes. In addition, for more severe symptoms, it may be helpful to refrain from sports and/or immobilize the area for a few weeks to help reduce the inflammation.
Recovery
This condition is self limiting, it will go away when the two parts of bony growth join together, this is natural. Unfortunately, Sever's disease can be very painful and limit sport activity of the child while waiting for it to go away, so treatment is often advised to help relieve it. In a few cases of Sever's disease, the treatment is not successful and these children will be restricted in their activity levels until the two growth areas join, usually around the age of 16 years. There are no known long term complications associated with Sever's disease.
Sever's disease, is a musculoskeletal condition occurring in adolescence that symptomatically manifests as posterior heel pain during ambulation. Often participation in physical activity is severely limited resulting in frustration for children and parents alike. Conservative treatment options have included rest, abstinence from athletic activity, heel lifts, foot orthotic devices, ice, and calf-stretching exercise. The authors are proposing arch taping as an additional viable treatment option for controlling heel pain during athletic and other weight-bearing activities in patients with Sever's disease.
Causes
Your child may have pain along the edges of one or both heels during exercise. The pain usually goes away with rest, but may be worse in the morning. Your child's heel may also be slightly swollen and warm. The heel pain may be worse when your child climbs steps or stands on tiptoe. It may cause your child to limp.
Symptoms
Pain in the bottom surface and at the back of the heel. Extreme pain when the child places their heel on the ground. The pain is aggravated when running or jumping on hard surfaces. The pain is reduced when the child walks or runs on their toes.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
In general, the goals for treatment include reducing the localized areas of inflammation. We recommend that patients utilize Ibuprofen every six to eight hours as needed. Stretching exercises on a daily basis, as well as prior to activity is thought to be helpful as well. Following work-outs and increased activities, it may be helpful to apply ice over affected areas. Heel cups are also available to provide cushion in shoes. In addition, for more severe symptoms, it may be helpful to refrain from sports and/or immobilize the area for a few weeks to help reduce the inflammation.
Recovery
This condition is self limiting, it will go away when the two parts of bony growth join together, this is natural. Unfortunately, Sever's disease can be very painful and limit sport activity of the child while waiting for it to go away, so treatment is often advised to help relieve it. In a few cases of Sever's disease, the treatment is not successful and these children will be restricted in their activity levels until the two growth areas join, usually around the age of 16 years. There are no known long term complications associated with Sever's disease.
Causes Signs Or Symptoms And Treating Of An Achilles Tendon Rupture
Overview
 An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.
An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.
Causes
The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms.
Symptoms
Ankle pain and swelling or feeling like the ankle has ?given out? after falling or stumbling. A loud audible pop when the ankle is injured. Patients may have a history of prior ankle pain or Achilles tendonitis, and may be active in sports. Swelling, tenderness and possible discoloration or ecchymosis in the Achilles tendon region. Indentation above the injured tendon where the torn tendon may be present. Difficulty moving around or walking. Individual has difficulty or is unable to move their ankle with full range of motion. MRI can confirm disruption or tear in the tendon. Inability to lift the toes.
Diagnosis
A physician usually can make this diagnosis with a good physical examination and history. X-rays usually are not taken. A simple test of squeezing the calf muscles while lying on your stomach should indicate if the tendon is still connected (the foot should point). This test isolates the connection between the calf muscle and tendon and eliminates other tendons that may still allow weak movement. A word of caution, Achilles tendon rupture is often misdiagnosed as a strain or minor tendon injury. Swelling and the continuing ability to weakly point your toes can confuse the diagnosis. Ultrasound and MRI are tests that can assist in difficult diagnosis. Depending on the degree of injury, these tests can also assist in determining which treatment may be best.
Non Surgical Treatment
Pain medicines can help decrease pain and swelling. A cast may be needed for 2 months or more. Your foot will be positioned in the cast with your toes pointing slightly down. Your caregiver will change your cast and your foot position several times while the tendon heals. Do not move or put weight on your foot until your caregiver tells you it is okay. A leg brace or splint may be needed to help keep your foot from moving while your tendon heals. Heel lifts are wedges put into your shoe or cast. Heel lifts help decrease pressure and keep your foot in the best position for your tendon to heal. Surgery may be needed if other treatments do not work. The edges of your tendon may need to be stitched back together. You may need a graft to patch the tear. A graft is a piece of another tendon or artificial material. 
Surgical Treatment
Most published reports on surgical treatment fall into 3 different surgical approach categories that include the following: direct open, minimally invasive, and percutaneous. In multiple studies surgical treatment has demonstrated a lower rate of re-rupture compared to nonoperative treatment, but surgical treatment is associated with a higher rate of wound healing problems, infection, postoperative pain, adhesions, and nerve damage. Most commonly the direct open approach involves a 10- to 18-cm posteromedial incision. The minimally invasive approach has a 3- to 10-cm incision, and the percutaneous approach involves repairing the tendon through multiple small incisions. As with nonsurgical treatment there exists wide variation in the reported literature regarding postoperative treatment protocols. Multiple comparative studies have been published comparing different surgical approaches, repair methods, or postoperative treatment protocols.
How To Check True Leg Length Discrepancy
Overview
There are generally two kinds of leg length discrepancies. Structural discrepancy occurs when either the thigh (femur) or shin (tibia) bone in one leg is actually shorter than the corresponding bone in the other leg. Functional discrepancy occurs when the leg lengths are equal, but symmetry is altered somewhere above the leg, which in turn disrupts the symmetry of the legs. For example, developmental dislocation of the hip (DDH) can cause a functional discrepancy. In DDH, the top of the leg bone (femur) that is not properly positioned in the hip socket may hang lower than the femur on the other side, giving the appearance and symptoms of a leg length discrepancy.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).

Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
There are generally two kinds of leg length discrepancies. Structural discrepancy occurs when either the thigh (femur) or shin (tibia) bone in one leg is actually shorter than the corresponding bone in the other leg. Functional discrepancy occurs when the leg lengths are equal, but symmetry is altered somewhere above the leg, which in turn disrupts the symmetry of the legs. For example, developmental dislocation of the hip (DDH) can cause a functional discrepancy. In DDH, the top of the leg bone (femur) that is not properly positioned in the hip socket may hang lower than the femur on the other side, giving the appearance and symptoms of a leg length discrepancy.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).
Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Acquired Flat Foot Surgery
Overview
Acquired adult flatfoot deformity (AAFD) is a progressive flattening of the arch of the foot that occurs as the posterior tibial tendon becomes insufficient. It has many other names such posterior tibial tendon dysfunction, posterior tibial tendon insufficiency and dorsolateral peritalar subluxation. This problem may progress from early stages with pain along the posterior tibial tendon to advanced deformity and arthritis throughout the hindfoot and ankle. 
Causes
Adult acquired flatfoot is caused by inflammation and progressive weakening of the major tendon that it is responsible for supporting the arch of the foot. This condition will commonly be accompanied by swelling and pain on the inner portion of the foot and ankle. Adult acquired flatfoot is more common in women and overweight individuals. It can also be seen after an injury to the foot and ankle. If left untreated the problem may result in a vicious cycle, as the foot becomes flatter the tendon supporting the arch structure becomes weaker and more and more stretched out. As the tendon becomes weaker, the foot structure becomes progressively flatter. Early detection and treatment is key, as this condition can lead to chronic swelling and pain.
Symptoms
In many cases, adult flatfoot causes no pain or problems. In others, pain may be severe. Many people experience aching pain in the heel and arch and swelling along the inner side of the foot.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery. 
Surgical Treatment
Surgical treatment should be considered when all other conservative treatment has failed. Surgery options for flatfoot reconstruction depend on the severity of the flatfoot. Surgery for a flexible flatfoot deformity (flatfoot without arthritis to the foot joints) involves advancing the posterior tibial tendon under the arch to provide more support and decrease elongation of the tendon as well as addressing the hindfoot eversion with a osteotomy to the calcaneus (surgical cut in the heel bone). Additionally, the Achilles tendon may need to be lengthened because of the compensatory contracture of the Achilles tendon with flatfoot deformity. Flatfoot deformity with arthritic changes to the foot is considered a rigid flatfoot. Correction of a rigid flatfoot deformity usually involves surgical fusion of the hindfoot joints. This is a reconstructive procedure which allows the surgeon to re-position the foot into a normal position. Although the procedure should be considered for advanced PTTD, it has many complications and should be discussed at length with your doctor.